Recording Death Administration
The Death Administration form is a quick and easy way to record the details required when a patient dies.
To record death administration:
- With the patient selected and an appropriate Encounter started, enter died in the .
- From Quick Entry Forms, select Death administration:
- The Death Administration screen displays:
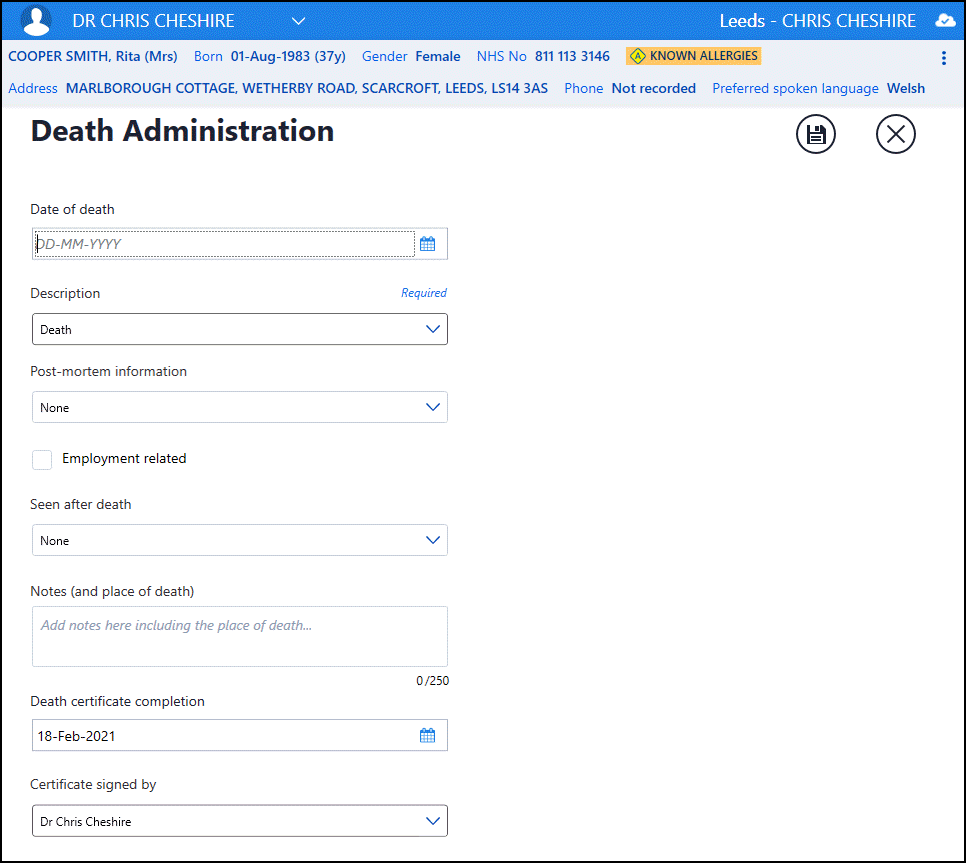
Complete as appropriate:
- Date of Death - Enter the date of the patient's death.
- Description - Defaults to Death, select from the clinical terms available if required.
- Date last seen alive - Enter a date if required.
- Post mortem information - Defaults to None, select from the list if appropriate.
- Employment related - Tick if the death is related to the patient's employment.
- Seen after death - Defaults to None, select from the list as appropriate.
- Notes (and place of death) - Enter any free text comments appropriate, up to a maximum of 250 characters.
- Death certificate completion - Defaults with today's date, update if required.
- Certificate signed by:
- If you are signed in as a clinician, this defaults to your details, update if appropriate.
- If you are not signed in as a clinician, this defaults to the patients Usual GP, or if there is no active Usual GP, their Registered GP. Update if appropriate.
- Shared Care Setting - Certificate signed by defaults to Other and cannot be updated.
- Select Save
 .
.
See Viewing Death Administration for further details.
Note - To print this topic select Print  in the top right corner and follow the on-screen prompts.
in the top right corner and follow the on-screen prompts.